| Back to Back Issues Page |
 |
|
Newsletter - New Secrets About Health and Wellness - Heart Attack, Stroke and Homocysteine November 03, 2013 |
Yours in Health and WellnessCholesterol or Homocysteine?Preventing Heart Attack and StrokeMany apologies for the duplication. But the subject line of your email did not get changed - my error and you might not have opened another newsletter on the GMO Mini Summit. Hence I am resending the issue on "Heart Attack, Stroke and Homocysteine". Damage to the arteries leading to coronary artery disease (CAD) or coronary vascular disease (CVD) is the primary route to heart attack and stroke. Cholesterol is the most popular culprit for arterial damage beginning with lesions, plaque deposit followed by endothelial dysfunction. But is it in reality the main culprit? 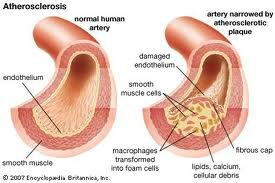
The build-up of plaque on the arterial walls increases the danger of plaque breaking off and causing a blockage leading to heart attack or stroke. If medical research could find a way to stop this process, or reverse it, or mitigate its effects the mortality rate from CAD/CVD would drop dramatically. It is an important issue because this process begins in young people. It is not a disease that begins with the elderly. In a 1998 study reported in the New England Journal of Medicine, a leading US medical journal, autopsies on 208 accident victims found lesions on artery walls and arterial fat deposits in: • 7% of those aged 2-15 • 33% of those 16-20 • 50% of those 21-25 • 70% of those 26-39 (N Engl J Med 1998: 338: 1650) I initially thought I could report on the main pieces of medical research in one Newsletter. But having reached 4 pages it is better to break it into three parts. This newsletter will examine homocysteine; the second will focus on cholesterol and related issues; and the third will look at various treatments. HomocysteineIn the mid-1960’s Dr. Thomas McCully, a graduate of Harvard Medical School was a young pathology instructor there. In his research he was puzzled by the cases of two young children who died from severe arteriosclerosis, what in lay terms we call hardening of the arteries – normally considered a disease of the elderly. Both children had homocystinuria a genetic disease which causes excessive blood levels of homocysteine. “By re-examining the autopsy tissues of both children and drawing on previous animal research, McCully emerged with two linked and provocative suggestions: perhaps homocysteine directly damages the cells and tissues of the arteries, in much the way that cholesterol is thought to do, and perhaps that damage occurs not just in these rare genetic cases but in the population at large, in any people with elevated homocysteine levels.” (NY Times Magazine 1997/08/10) -opens in new window.Cholesterol had been referenced in 1913 as a cause of cardio-vascular disease (CVD) by a Russian scientist who had fed purified cholesterol to rabbits. Over the next 60 years, especially post-WW2, the cholesterol theory of CVD very slowly became more accepted by the medico-scientific community. McCully in enlarging his hypothesis about homocysteine as a causative factor for CVD observed that Vitamins B6, B12, and folic acid when administered to animals quickly lowered levels of homocysteine to the normal range. He suggested that the same was true for humans. So if this was such an important finding why did homocysteine disappear from the debate? Two factors worked against McCully. Unfortunately for him not even one of these natural substances could be patented by a pharmaceutical company; therefore no big money could be made by Big Pharma; therefore no research dollars from Big Pharma. Simultaneously research on cholesterol, the competing theory for the cause of CVD, was discovering synthetic substances that would lower blood levels of cholesterol. And these synthetic substances could be patented.Big bucks could be made; therefore research funding was available. So lots of research money for cholesterol; none for homocysteine. McCully’s research funding dried up; he was ostracized and pushed out of Harvard while the research dollars shifted to cholesterol and patentable cholesterol lowering drugs. In commenting, years later in 1997, on this situation “Thomas N. James, a cardiologist and president of the University of Texas Medical Branch who was also the president of the American Heart Association in 1979 and '80, is even harsher. ‘It was worse than that you couldn't get ideas funded that went in other directions than cholesterol,’ he says. ‘You were intentionally discouraged from pursuing alternative questions. I've never dealt with a subject in my life that elicited such an immediate hostile response’.''( NY Times Mag 1997/08/10) So McCully and homocysteine were sidelined for 25 critical years – until about the mid-1990s. Homocysteine Makes A ComebackBy 1994 researchers could safely assert that “Increased levels of plasma homocysteine are generally accepted as one of the causes leading to arteriosclerosis and thromboembolism”. In their study they found that 72 of 309 patients under age 50 and suffering from arterial blockage had elevated homocysteine. They were treated daily with 250 mg vitamin B6 and 5 mg folic acid. After 6 weeks 6 of the 72 patients still had mild elevated homocysteine. Continued treatment with B6 and folic acid normalized the homocysteine levels in over 90% of them. (.J Vascular Surg 1994; 20(6):933-40) The following year the Journal of the American Medical Association reported that in a review of 27 previously published studies, researchers concluded that increasing levels of homocysteine were an independent risk factor for coronary artery disease, stroke and peripheral vascular disease. The overwhelming majority of patients with increased homocysteine had nutritional deficiencies of folic acid and Vitamins B6 and B12 . (JAMA 1995; 1049-1057) Despite this and other similar findings, few people have ever had their homocysteine levels checked and very few doctors prescribe such tests. You should insist on this test along with a check of your Cholesterol and triglycerides. The same year it was reported that if we take 1000 mcg of folic acid along with Vitamins B6and B12 in supplementation each day, 92% of homocysteine levels would fall to a safe range. (Lancet 1995; (345):85-89) The evidence continued to pile up. In 1997 one study found a nine fold increase in cardiovascular risk when homocysteine levels exceeded 20 umol/L. (N Engl J Med 1997; July 24) In a highly technical study of 17 healthy volunteers (10 males and 7 females aged 21-59) it was found that elevation in plasma homocysteine is associated with an acute impairment of vascular endothelial function. This can be prevented by pre-treatment with vitamin C in healthy subjects. The scientists concluded that the adverse effects of homocysteine on vascular endothelial cells are mediated through oxidative stress mechanisms.(Circulation 1999; 1156-60) A British study demonstrated that supplementation with folic acid and vitamin B6 improved biological markers of endothelial injury, the principal cause of premature atherosclerosis and venous thromboembolic disease. (Br J Haemotology 1999; 107:776-8) In 1999 a meta-analysis conclusively established the relationship between elevated homocysteine levels hyperhomocystinemia) and cardiovascular disease. (Cardiologia 1999;44:627-31) In a randomized, placebo-controlled trial among 158 healthy siblings of 167 patients with premature atherothrombotic disease, 80 were assigned placebo and 78 were assigned 5 mg folic acid with 250 mg Vitamin B6 daily for 2 years. There was a significant decrease in homocysteine levels in those using B6 and folic acid and they had a decreased rate of abnormal exercise electrocardiography tests – which is consistent with a decreased risk of atherosclerotic coronary events. (Lancet 2000; 355(9203):517-22 The evidence continued to grow. In 2001 Spence et al noted that elevated levels of homocysteine are surprisingly common and strongly associated with endothelial dysfunction. Such elevated levels have emerged as a risk factor for stroke and cardiovascular disease. Treatment with a combination of folic acid, pyridoxine (Vitamin B6) and cobalamin (Vitamin B12) reduces plasma homocysteine levels and in most cases restores endothelial function and causes regression in plaque in the carotid artery for stroke prevention. (Neuroepidemiology 2001;20:16-25) Another study, reported in the British Medical Journal, estimated that reducing homocysteine by 3 umol/L is associated with risk reduction of 24% for stroke and 16% for ischemic heart disease. They also suggested that folic acid, pyridoxine (B6) and cobalamin (B12) reduce plasma homocysteine levels and may lead to regression of plaque.(BMJ 2002; Nov 23) And may lead to regression of plaque. Isn't that fascinating? Another British medical journal in 2005 noted the role of homocysteine in increasing the risk for diabetes and coronary issues. The authors reported that South Asians (persons of Pakistani, Indian or Bangladeshi origin) develop diabetes 5-10 years earlier than Europeans and have a greater risk of coronary heart disease (CHD) attributable in part to insulin resistance, central adiposity, increased subclinical inflammation and thrombogenic tendency and higher homocysteine levels. “After immigration, the adoption of a western diet allied to increasingly sedentary behaviour leads to weight gain, hypertension, hyperlipidaemia” contributing to higher rates of CHD.(Br J Diabetes Vasc Dis 2005; 5(5) 253-259) A Chinese study examined 237 consecutive patients undergoing a coronary angiogram. 138 patients were identified by angiogram as having coronary artery disease (CAD) while 99 patients had normal coronary angiogram. In comparing homocysteine levels in each group, while controlling for other factors Ni et al found “a high homocysteine level is an independent and important risk factor of CAD and the relative risk of CAD conferred by homocystinemia is similar to that of dyslipidemia in the Chinese population at high risk of CAD”. (Am J Cardiol 2007 Aug 1;100(3):455-8) An important note – vegetarians have difficulty with higher total homocysteine levels and have lower levels of Vitamin B12 according to a 2002 study by L Bissoli et al. (Ann Nutr Metab 2002;46:73–79) Supplementation is needed. The evidence for the link between elevated levels of homocysteine and endothelial dysfunction and ultimately cardiovascular disease is compelling, to say the least. The medical research is overwhelmingly clear that elevated homocysteine can be effectively brought to a normal level through the use of Vitamins B6 and 12 along with 1000 mcg of folic acid. Quality nutritional supplements like USANA’s Essentials (new window) contain these ingredients..Do you know your homocysteine level? In the next Newsletter we’ll look at the medical evidence on cholesterol and its reputed role in CAD/CVD. We’ll also look at the different types of cholesterol. Do they all have the same impact on your cardiovascular health? Yours in health and wellness, Roger |
| Back to Back Issues Page |